
Articles
- Page Path
- HOME > Korean J Community Nutr > Volume 31(2); 2026 > Article
-
Review
- Life-course personalized nutrition strategy for adolescents and young adults in Korea based on a behavioral science approach and community-based model: a narrative review
-
Jung-Hyun Kim†

-
Korean Journal of Community Nutrition 2026;31(2):127-139.
DOI: https://doi.org/10.5720/kjcn.2026.00129
Published online: April 30, 2026
Professor, Department of Food and Nutrition, Pai Chai University, Daejeon, Korea
- †Corresponding author: Jung-Hyun Kim Department of Food and Nutrition, Pai Chai University, 155-40 Baejae-ro, Seo-gu, Daejeon 35345, Korea Tel: +82-42-520-5424 Fax: +82-70-4850-8485 Email: jhkim99@pcu.ac.kr
• Received: April 8, 2026 • Revised: April 22, 2026 • Accepted: April 23, 2026
© 2026 The Korean Society of Community Nutrition
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 743 Views
- 15 Download
- Abstract
- INTRODUCTION
- METHODS
- STRATEGIC IMPORTANCE OF ADOLESCENCE AND YOUNG ADULTHOOD: THEORETICAL RATIONALE
- CURRENT NUTRITIONAL STATUS AND KEY NUTRITIONAL CHALLENGES IN KOREAN ADOLESCENTS AND YOUNG ADULTS
- THE SCHOOL-TO-SOCIETY NUTRITION GAP: A STRUCTURAL ANALYSIS
- BEHAVIORAL SCIENCE FRAMEWORKS FOR NUTRITIONAL BEHAVIOR
- IMPLEMENTATION AND LIMITATIONS OF COMMUNITY-BASED NUTRITION STRATEGIES
- A LIFE-COURSE PERSONALIZED COMMUNITY NUTRITION STRATEGY MODEL
- CONCLUSIONS
- NOTES
- REFERENCES
Abstract
-
Objectives
- This review examines the nutritional challenges among Korean adolescents and young adults from life-course and behavioral science perspectives and proposes an integrated, community-based nutrition strategy for this critical transitional period.
-
Methods
- A narrative review was conducted following the Scale for the Quality Assessment of Narrative Review Articles guidelines. Literature published between January 2015 and June 2025 was retrieved from PubMed, Google Scholar, and Research Information Sharing Service using keywords related to adolescent and young adult nutrition, life course approaches, behavioral nutrition, and personalized nutrition. Policy documents from the World Health Organization, Food and Agriculture Organization of the United Nations, United Nations Nutrition, and Korean government agencies were also included. A total of 40 references (32 peer-reviewed articles and 8 policy reports) were analyzed.
-
Results
- Korean adolescents and young adults exhibited high rates of skipping breakfast (> 38.3%), obesity, and excessive sodium and sugar intakes, with disparities driven by socioecological determinants. The Developmental Origins of Health and Disease framework highlights adolescence as the “second window of plasticity” for reshaping long-term health trajectories. Two behavioral frameworks were synthesized: the Formation–Maintenance Model, distinguishing adolescent (Learn–Practice) and young adult (Sustain) stages, and the socioecological nutrition model, addressing multi-level influences on dietary behavior. A structural discontinuity in public nutrition support, termed the “School-to-Society Nutrition Gap,” was identified. Community-based, participatory, and digitally integrated interventions showed strong potential for sustaining behavioral change.
-
Conclusion
- A personalized life-course nutrition strategy based on a Learn-Practice-Sustain framework was proposed. A Community-Linked Circular Nutrition Model was presented to bridge the gap between school-based and community-level nutrition systems, emphasizing nutrition equity and digital engagement as key drivers of sustainable health outcomes.
INTRODUCTION
METHODS
STRATEGIC IMPORTANCE OF ADOLESCENCE AND YOUNG ADULTHOOD: THEORETICAL RATIONALE
CURRENT NUTRITIONAL STATUS AND KEY NUTRITIONAL CHALLENGES IN KOREAN ADOLESCENTS AND YOUNG ADULTS
THE SCHOOL-TO-SOCIETY NUTRITION GAP: A STRUCTURAL ANALYSIS
BEHAVIORAL SCIENCE FRAMEWORKS FOR NUTRITIONAL BEHAVIOR
IMPLEMENTATION AND LIMITATIONS OF COMMUNITY-BASED NUTRITION STRATEGIES
A LIFE-COURSE PERSONALIZED COMMUNITY NUTRITION STRATEGY MODEL
CONCLUSIONS
-
CONFLICT OF INTEREST
There are no financial or other issues that might lead to conflict of interest.
-
FUNDING
None.
-
ACKNOWLEDGEMENTS
This study was based on a presentation delivered at the 2025 Fall Conference of the Korean Society of Community Nutrition.
-
DATA AVAILABILITY
This narrative review is based on previously published literature and does not contain original data.
NOTES
Fig. 1.Community-linked circular nutrition model for adolescents and young adults, illustrating the integration of life-course stages, community-linked ecosystems, and core implementation principles.
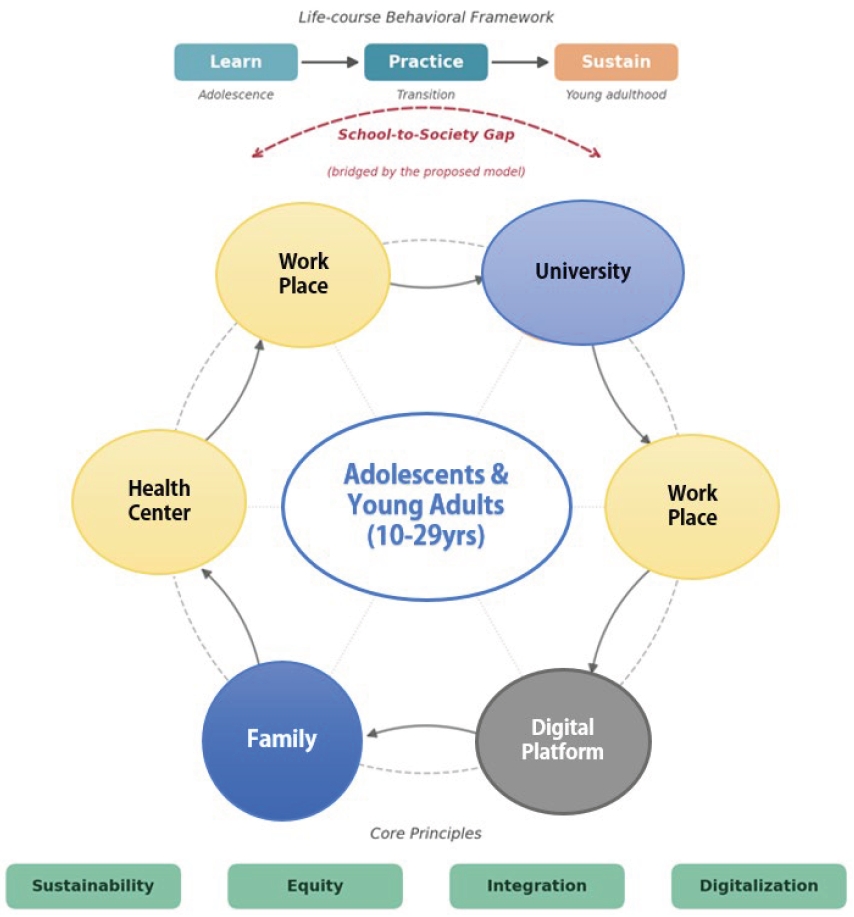
Table 1.Major nutrition risk indicators among Korean adolescents and young adults
Based on Korea Disease Control and Prevention Agency [14].
WHO, World Health Organization.
Table 2.Paradigm shift in adolescent and young adult nutrition: past, present, and future
- 1. UN-Nutrition. UN-Nutrition strategy 2022–2030: one UN for nutrition [Internet]. UN-Nutrition; 2022 [cited 2025 Jun 1]. Available from: https://www.unnutrition.org/wp-content/uploads/UN-Nutrition-Strategy-2022-2030_WEB_28Oct2022_EN.pdf
- 2. World Health Organization (WHO). Global action plan for the prevention and control of noncommunicable diseases 2013–2020 [Internet]. WHO; 2013 [cited 2025 Jun 1]. Available from: https://www.who.int/publications/i/item/9789241506236
- 3. Sobal J, Bisogni CA. Constructing food choice decisions. Ann Behav Med 2009; 38 Suppl 1: S37-S46. ArticlePubMed
- 4. Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet 2016; 387(10036): 2423-2478. ArticlePubMedPMC
- 5. Puri S, Shaheen M, Grover B. Nutrition and cognitive health: a life course approach. Front Public Health 2023; 11: 1023907.ArticlePubMedPMC
- 6. Moore Heslin A, McNulty B. Adolescent nutrition and health: characteristics, risk factors and opportunities of an overlooked life stage. Proc Nutr Soc 2023; 82(2): 142-156. ArticlePubMed
- 7. Hargreaves D, Mates E, Menon P, Alderman H, Devakumar D, Fawzi W, et al. Strategies and interventions for healthy adolescent growth, nutrition, and development. Lancet 2022; 399(10320): 198-210. ArticlePubMed
- 8. Azzopardi PS, Hearps SJC, Francis KL, Kennedy EC, Mokdad AH, Kassebaum NJ, et al. Progress in adolescent health and wellbeing: tracking 12 headline indicators for 195 countries and territories, 1990–2016. Lancet 2019; 393(10176): 1101-1118. ArticlePubMedPMC
- 9. Gluckman PD, Hanson MA, Buklijas T. A conceptual framework for the developmental origins of health and disease. J Dev Orig Health Dis 2010; 1(1): 6-18. ArticlePubMed
- 10. Hanson MA, Gluckman PD. Early developmental conditioning of later health and disease: physiology or pathophysiology? Physiol Rev 2014; 94(4): 1027-1076. ArticlePubMedPMC
- 11. Hanson MA, Gluckman PD. Developmental origins of health and disease: new insights. Basic Clin Pharmacol Toxicol 2008; 102(2): 90-93. ArticlePubMed
- 12. Baethge C, Goldbeck-Wood S, Mertens S. SANRA—a scale for the quality assessment of narrative review articles. Res Integr Peer Rev 2019; 4: 5.ArticlePubMedPMCPDF
- 13. Sukhera J. Narrative reviews: flexible, rigorous, and practical. J Grad Med Educ 2022; 14(4): 414-417. ArticlePubMedPMCPDF
- 14. Korea Disease Control and Prevention Agency (KDCA). Korea Health Statistics 2023: Korea National Health and Nutrition Examination Survey (KNHANES Ⅸ-2). KDCA; 2025 [cited 2025 Dec 22]. Available from: https://knhanes.kdca.go.kr
- 15. Barker DJ. The fetal and infant origins of adult disease. BMJ 1990; 301(6761): 1111.ArticlePubMedPMC
- 16. World Health Organization (WHO). Adolescent and young adult health [Fact sheet] [Internet]. WHO; 2024 [cited 2025 Jun 1]. Available from: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions
- 17. Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol 2000; 55(5): 469-480. ArticlePubMed
- 18. Chong MF. Dietary trajectories through the life course: opportunities and challenges. Br J Nutr 2022; 128(1): 154-159. ArticlePubMed
- 19. Arlinghaus KR, Stang JS. Population-engaged approaches to improving adolescent nutrition. J Nutr 2021; 151(6): 1371-1372. ArticlePubMedPDF
- 20. Tohi M, Bay JL, Tu’akoi S, Vickers MH. The developmental origins of health and disease: adolescence as a critical lifecourse period to break the transgenerational cycle of NCDs. Int J Environ Res Public Health 2022; 19(10): 6024.ArticlePubMedPMC
- 21. Øverby NC, Hillesund ER, Medin AC, Vik FN, Ostojic SM. Nutrition in a lifecourse perspective: from molecular to social determinants. Matern Child Nutr 2024; 20(Suppl 2): e13582. ArticlePubMed
- 22. Tohi M, Tu’akoi S, Vickers MH. A systematic review exploring evidence for adolescent understanding of concepts related to the developmental origins of health and disease. J Dev Orig Health Dis 2023; 14(6): 755-762. ArticlePubMed
- 23. Nagata JM, Helmer CK, Wong J, Diep T, Domingue SK, Do R, et al. Social epidemiology of early adolescent nutrition. Pediatr Res 2025; 98(3): 885-894. ArticlePubMedPMCPDF
- 24. Wolfson JA, Insolera N, Laska MN, Leung CW. High prevalence of food insecurity and related disparities among US college and university students from 2015–2019. J Nutr Educ Behav 2024; 56(1): 27-34. ArticlePubMedPMC
- 25. Kim DJ, Lee SB, Choi JH, Son SO. Young adult health behavior and policy challenges. Korea Institute for Health and Social Affairs; 2025. Report No. 2025-29.
- 26. Food and Agriculture Organization (FAO). Influencing food environments for healthy diets [Internet]. FAO; 2016 [cited 2025 Jun 1]. Available from: https://openknowledge.fao.org/items/060ce716-3d8b-4574-9857-dc38252fc283
- 27. Korean Law Information Center. School meals act, article 5, paragraph 1 [Internet]. Ministry of Government Legislation; 2026 [cited 2026 Apr 22]. Available from: https://www.law.go.kr/LSW/lsInfoP.do?lsiSeq=283421
- 28. Ministry of Agriculture, Food and Rural Affairs (MAFRA). The 4th basic plan for dietary life education (2025–2029). [Internet]. MAFRA; 2025 [cited 2025 Jun 1]. Available from: https://www.mafra.go.kr/bbs/home/792/586259/download.do
- 29. Winpenny EM, van Sluijs EMF, White M, Klepp KI, Wold B, Lien N. Changes in diet through adolescence and early adulthood: longitudinal trajectories and association with key life transitions. Int J Behav Nutr Phys Act 2018; 15(1): 86.ArticlePubMedPMCPDF
- 30. Utter J, Larson N, Laska MN, Winkler M, Neumark-Sztainer D. Self-perceived cooking skills in emerging adulthood predict better dietary behaviors and intake 10 years later: a longitudinal study. J Nutr Educ Behav 2018; 50(5): 494-500. ArticlePubMedPMC
- 31. Nam Y, Yoon J, Kim M. Application of draft nutritional standards for school lunches in the Republic of Korea: a feasibility study from the supplier perspective. Nutr Res Pract 2023; 17(1): 149-163. ArticlePubMedPMCLink
- 32. United Nations Children’s Fund (UNICEF). Undernourished and overlooked: a global nutrition crisis in adolescent girls and women [Internet]. UNICEF; 2023 [cited 2026 Apr 22]. Available from: https://www.unicef.org/reports/undernourished-overlooked-nutrition-crisis/
- 33. Nakabayashi J, Melo GR, Toral N. Transtheoretical model-based nutritional interventions in adolescents: a systematic review. BMC Public Health 2020; 20(1): 1543.ArticlePubMedPMCPDF
- 34. World Health Organization (WHO). Global accelerated action for the health of adolescents (AA-HA!): guidance to support country implementation, second edition. WHO; 2023.
- 35. Perski O, Blandford A, West R, Michie S. Conceptualising engagement with digital behaviour change interventions: a systematic review using principles from critical interpretive synthesis. Transl Behav Med 2017; 7(2): 254-267. ArticlePubMedPMCPDF
- 36. Kim M, Kim SY, Yoon J. Study on necessity of updating nutritional standards for school lunch programs in Korea. J East Asian Soc Diet Life 2017; 27(2): 137-147.
- 37. Sari DN, Hilmanto D, Sunjaya DK, Sari P. Community-based interventions to improve adolescent nutrition: a scoping review. BMC Public Health 2025; 25(1): 4615.ArticlePubMedPMCPDF
- 38. Ranisavljev M, Kurniawan AL, Ferrero E, Shinde S, Zhao S, Partap U, et al. Community-based interventions addressing multiple forms of malnutrition among adolescents in low- and middle-income countries: a scoping review. Nutr J 2025; 24(1): 69.ArticlePubMedPMC
- 39. Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S, et al. Food in the Anthropocene: the EAT-Lancet commission on healthy diets from sustainable food systems. Lancet 2019; 393(10170): 447-492. ArticlePubMed
- 40. United States Department of Agriculture (USDA). USDA announces actions on nutrition security [Internet]. USDA; 2022 [cited 2025 Jun 1]. Available from: https://www.usda.gov/media/press-releases/2022/03/17/usda-announces-actions-nutrition-security
- 41. Laska MN, Larson NI, Neumark-Sztainer D, Story M. Does involvement in food preparation track from adolescence to young adulthood and is it associated with better dietary quality? Findings from a 10-year longitudinal study. Public Health Nutr 2012; 15(7): 1150-1158. ArticlePubMedPMC
- 42. Escobedo-Monge M, Lustig RH, Suchkov S, Blokh S, Andronova N, Goryacheva O, et al. Personalized nutrition in pediatric chronic diseases. Metabolites 2025; 15(10): 653.ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteLife-course personalized nutrition strategy for adolescents and young adults in Korea based on a behavioral science approach and community-based model: a narrative review
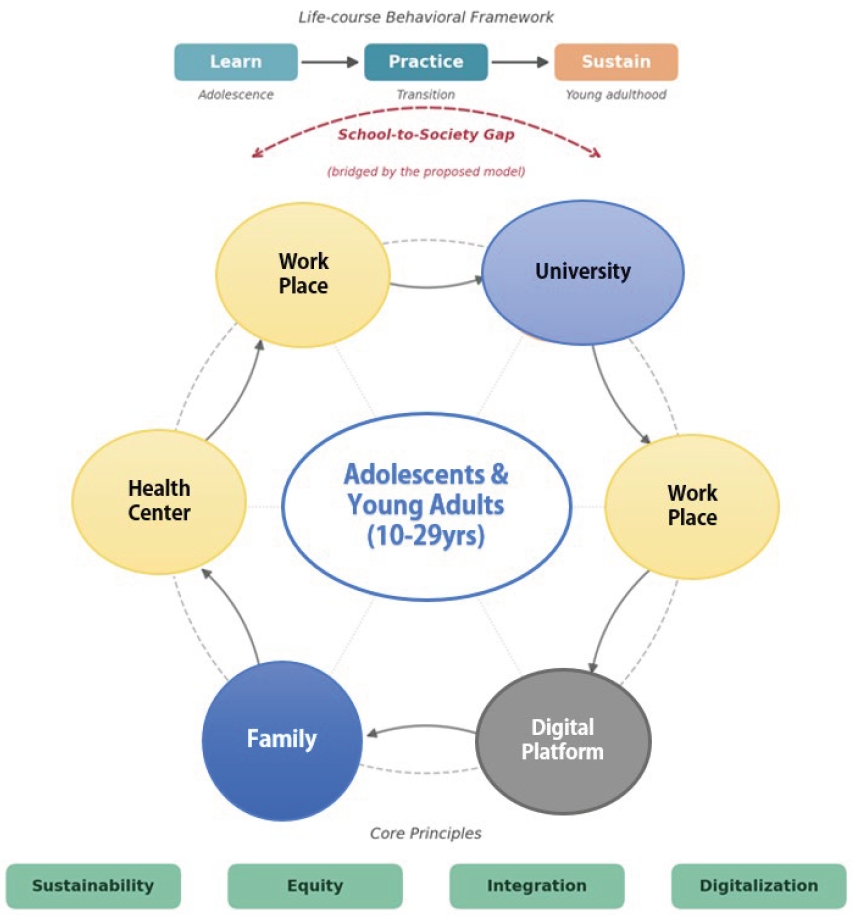
Fig. 1. Community-linked circular nutrition model for adolescents and young adults, illustrating the integration of life-course stages, community-linked ecosystems, and core implementation principles.
Fig. 1.
Life-course personalized nutrition strategy for adolescents and young adults in Korea based on a behavioral science approach and community-based model: a narrative review
| Indicator | Adolescents (10–19 years) | Young adults (20–29 years) | Interpretation |
|---|---|---|---|
| Breakfast skipping | 38.3% (2023) | 40.3% (2023) | Irregular eating patterns and increased risk of nutritional imbalance |
| Obesity prevalence | 16.2% (middle/high school, 2023) | 29.6% (2023) | Continuous increase over the past decade; higher prevalence in males |
| Sodium intake | 2,950 mg (exceeding WHO limit of 2,000 mg/day) | 3,204 mg (exceeding WHO limit of 2,000 mg/day) | Associated with processed foods and food delivery consumption |
| Era | Key characteristics | Policy and academic focus | Keywords | Strategic direction |
|---|---|---|---|---|
| Past | Deficiency prevention | Nutrient intake, school meals, growth | Quantity/deficiency | How much to eat (supply-focused) |
| Present | Food environment and overnutrition focus | Food environment, behavioral economics, digital tools | Environment/overnutrition | What, why, and how to eat |
| Future | Sustainability- and equity-focused | Nutrition security, sustainable diets, AI-based coaching | Sustainability/equity | Personalized nutrition coaching |
Table 1. Major nutrition risk indicators among Korean adolescents and young adults
Based on Korea Disease Control and Prevention Agency [ WHO, World Health Organization.
Table 2. Paradigm shift in adolescent and young adult nutrition: past, present, and future
Based on Willett AI, artificial intelligence.


